Alexander C. MettingVanRijn, Anthony P. Kuiper, Taco E. Dankers and Cees A. Grimbergen.
Academic Medical Center, Medical Physics Department, Meibergdreef 15 1105 AZ Amsterdam, The Netherlands.
Abstract- The accepted models of the origin of interference in body surface potential recordings predict that it would be advantageous to perform signal amplification on the electrode. A suitable circuit for a miniature biopotential amplifier to be manufactured in thick-film technology is described. A prototype series of active electrodes was produced and tested. The high immunity to interference resulted in ECG and EEG recordings of a very high quality.I. INTRODUCTION
Another problem with the passive electrodes in modern biopotential measurement systems originates from the current trend to combine low-noise analog circuitry and fast logic in the front-end. It was argued in an earlier paper that optimal instrumentation in terms of interference rejection and patient-safety should consist of a small battery powered front-end with a fiber-optic connection to the signal-processing hard-ware (usually a PC) [2]. With currently available components, the best solution is to perform the analog to digital conver-sion in the isolated front-end and to use a digital transmission format for the fiber-optic transmission link. A consequence of such a setup is, however, that special attention has to be paid to the problem of interference from the digital circuitry coupled into the sensitive analog input circuitry.
The two described problems could in principle be solved if the analog signal processing would be performed at the electrode. Such an active transducer would form a signal source with a low output impedance which would eliminate the need for shielded wires. In addition, proper shielding of the digital circuitry with respect to the analog input amplifiers would be feasible.
II. METHODS
The main design goals were to keep the size and costs of the electrode comparable to a standard EEG electrode. The cost factor eliminated the possibility of a custom made integrated circuit. We found a good alternative in combining thick-film technology with an amplifier design developed by our group to be used with a minimal number of parts [4]; the circuitdiagram is shown in Fig. 1
. 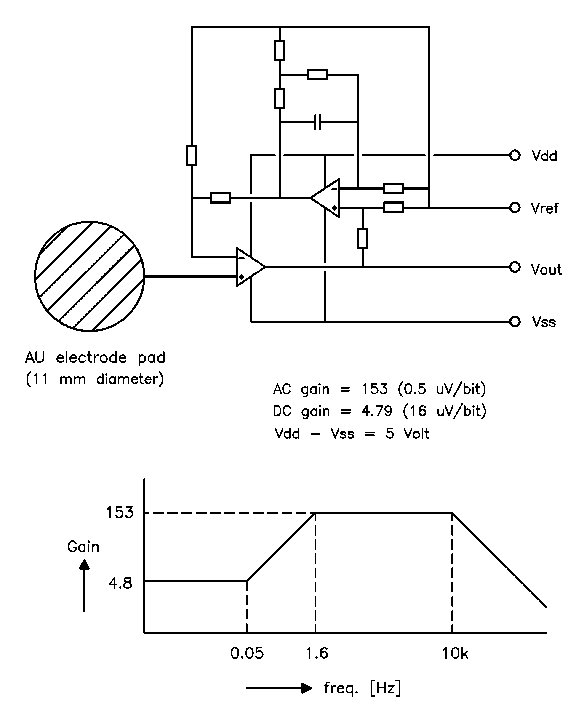
Fig. 1 The circuit diagram and transfer function of the active electrode. The stopped integrator in the feedback loop reduces the gain for low frequencies in order to keep the relatively large electrode offset voltages within the dynamic range of a 16 bit ADC.
 |
Active electrode, first experimental version
|
The electronic components are mounted at one side of a ceramic substrate with a diameter of 11 mm, while the other side is covered with a printed gold layer to form the electrode surface. The electronics are sealed with epoxy. The electrode is equipped with a 4 lead ribbon wire of 1 meter length with a small low-cost crimp connector. No expensive components or production processes have been used.
III. RESULTS
IV. DISCUSSION
Production costs were kept minimal by using only well established thick-film production techniques and by designing the electronics around easily available standard components (1 dual opamp in naked chip version, 8 SMD metal-film resistors and 1 SMD capacitor). The projected production costs for large series is in the order of US$ 10. Some practical details need further improving. The current used ribbon cable is cheap and easily mounted with a connector but not really flexible enough for day-to-day clinical use. Another point of further research is the combination of the chosen electrode material and the various electrode pastes which at the moment is the limiting factor for the signal quality.
V. CONCLUSIONS
AKNOWLEDGEMENTS
REFERENCES
[2] A. C. MettingVanRijn, A. P. Kuiper, A. C. Linnenbank and C. A. Grimbergen, "Patient isolation in multichannel bioelectric recordings by digital transmission through a single optical fiber," IEEE Trans. Biomed. Eng., vol. 40, pp. 302-308, 1993.
[3] F. Z. Padmadinata, J. J. Veerhoek, G. J. A. Van Dijk and J. H. Huijsing, "Microelectronic skin electrode," Sensors and Actuators, vol. B1, pp. 491-494, 1990.
[4] A. C. MettingVanRijn, A. Peper and C. A. Grimbergen, "Amplifiers for bioelectric events: a design with a minimal number of parts". Med. & Biol. Eng. & Comput., vol. 32, pp. 305-310, 1994. Fig. 2 An EEG signal measured with the active electrodes on the unprepared skin. Note the low noise level of approx 3 æVpk-pk and the absence of 50 Hz interference.
Hiç yorum yok:
Yorum Gönder